The Dizziness Spectrum: How ICD-10 R42 Guides the Clinician Through the Grey Zone

May 12, 2026
Dizziness is a subjective symptom, not a diagnosis. Yet it is among the most common presenting complaints in clinical medicine, and it frequently lands in the mental health clinician's office—often after a patient has exhausted the medical work‑up and been told “nothing is wrong.”
For the therapist, the diagnostic task is not to locate the precise neuro‑otological lesion but to determine where on the spectrum between organic and psychological dizziness a particular patient falls. The ICD‑10‑CM code for dizziness and giddiness is R42, but using it correctly requires understanding what it includes, what it explicitly excludes, and how it interacts with psychiatric diagnoses. This article examines the clinical architecture of dizziness coding, the distinction between vertiginous and non‑vertiginous presentations, and the documentation strategies that distinguish a primary psychiatric disorder from a symptom in search of an aetiology.
R42: The Symptom Code Without a Solution
The ICD‑10‑CM code R42 (Dizziness and giddiness) is a billable, specific code that can be used for reimbursement purposes. It falls within the Chapter 18 range R40‑R46 (Symptoms and signs involving cognition, perception, emotional state and behavior)—codes that describe what the patient experiences when the underlying cause is not yet known or when the symptom is not attributable to a specific disease. The 2026 edition of R42 became effective on 1 October 2025, and the code is valid for all HIPAA‑covered transactions from 1 October 2025 through 30 September 2026.
R42 is explicitly described as applying to “light‑headedness” and “vertigo”, but crucially it is used when the patient‘s complaint is general dizziness and the cause remains unspecified. The code functions as a placeholder—a way to document that the patient is experiencing the symptom while the diagnostic work‑up continues or when the symptom is not part of a recognised disease pattern. It is the code of clinical humility.
The code‘s “Applicable To” terms include both “dizziness” and “giddiness”, but note that “vertigo NOS (not otherwise specified)” also falls under R42 when no specific vestibular diagnosis has been established. This is a point of frequent confusion: vertigo as a symptom can be coded with R42, but vertigo as a confirmed diagnosis (e.g., benign paroxysmal positional vertigo) requires a code from Chapter 6 (Diseases of the nervous system), specifically H81.1‑ (Benign paroxysmal vertigo) or other codes in the H81 range.
The official Excludes2 notes for R42 are clinically instructive:
Excludes2: psychogenic dizziness (F45.8) – Other somatoform disorders
Excludes2: vertigo NOS (H81.9) – Unspecified disorder of vestibular function
These are Excludes2 notes, meaning the conditions are not part of R42 and can be used together with R42 if the patient has both diagnoses. However, once a specific organic cause is identified (e.g., BPPV, vestibular neuritis, Ménière‘s disease), the specific code from Chapter 6 should replace R42 as the principal diagnosis.
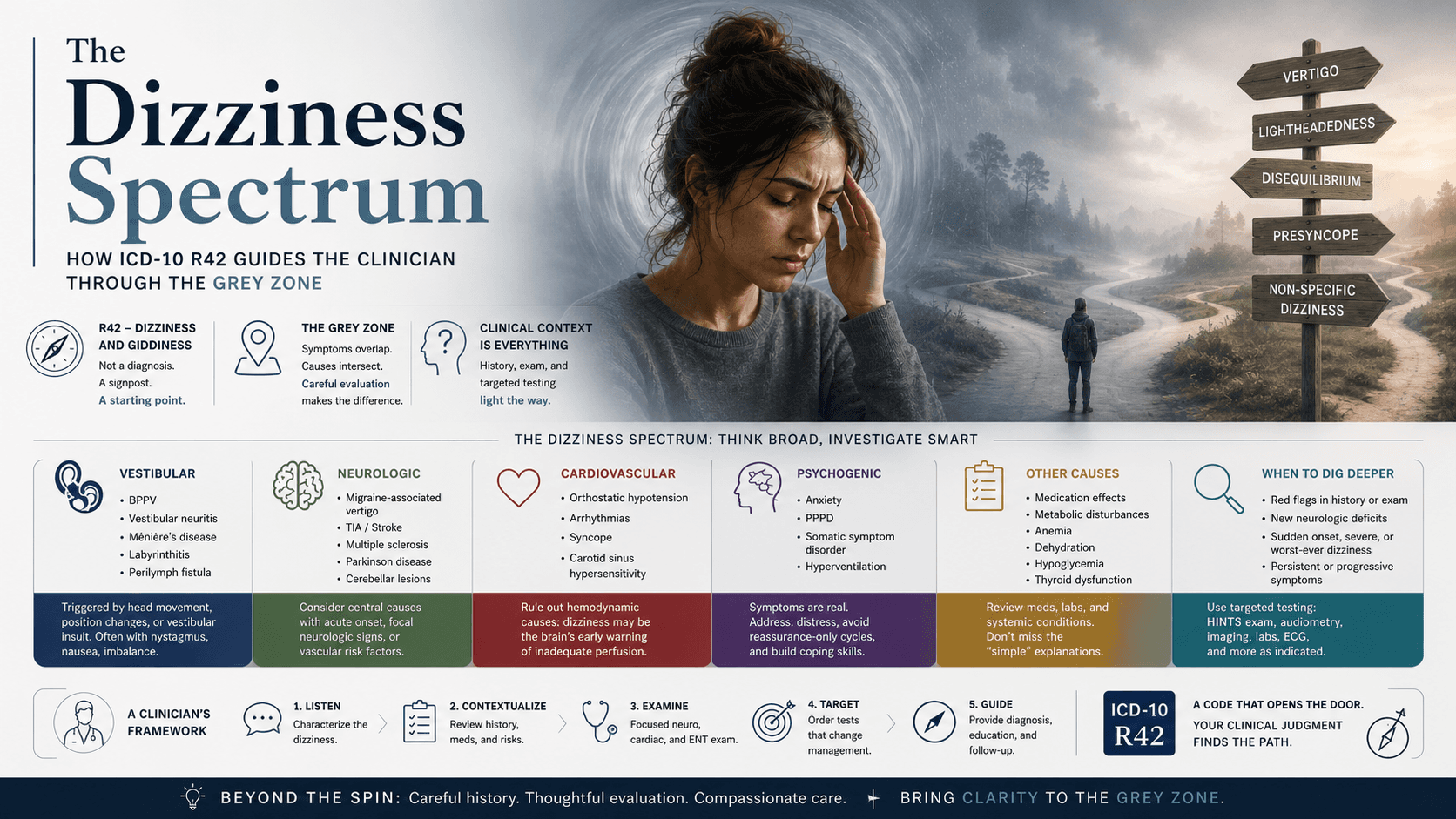
The Typology of Dizziness: Vertigo, Light‑Headedness, Disequilibrium
The Excludes2 notes are not arbitrary; they reflect a deeper clinical reality. Dizziness is not a single sensation. The four recognised subtypes each point toward different aetiologies:
1. Vertigo is the illusion of movement—spinning, tilting, or swaying—caused by asymmetric involvement of the vestibular system. It is the most common type of dizziness, defined as an illusion of movement that may involve the perception of self‑motion or the motion of the environment. Central causes include cerebrovascular disorders (vertebrobasilar circulation), migraine, multiple sclerosis, posterior fossa tumours, neurodegenerative disorders, some drugs, and psychiatric disorders.
2. Light‑headedness is a feeling of faintness or being on the verge of syncope, without the sensation of movement. It differs fundamentally from vertigo. The ICD‑10‑CM code for light‑headedness is R42.81, a more specific subcode that distinguishes this sensation from general dizziness. Light‑headedness often points to cardiovascular causes (orthostatic hypotension, arrhythmias) or hyperventilation.
3. Disequilibrium is a sensation of unsteadiness or imbalance when standing or walking, often without a subjective sense of spinning. It falls under R42 when no specific cause is identified.
4. Presyncope is the sensation of impending faint without loss of consciousness. It is coded separately with codes from Chapter 9 (Diseases of the circulatory system) when a cardiovascular cause is established.
For the mental health clinician, the critical distinction is between vertigo (which suggests a vestibular or central neurological process) and light‑headedness or non‑specific giddiness (which is the typical presentation of hyperventilation, anxiety, or panic). A patient who describes “the room spinning” has a different differential than a patient who describes “feeling like I might faint.”
The Dizziness‑Anxiety Loop: When Psychiatric Disorder Masquerades as Vestibular Disease
The relationship between dizziness and psychiatric disorder is bidirectional and often circular. A 2008 BMJ article noted a common clinical pattern: patients develop dizziness that they represent as vertigo, but in fact it is usually the onset of an anxiety state (generalised anxiety disorder) for a variety of reasons, in which balance discomfort predominates. Years later, they suddenly develop ‘dizziness‘ which they represent as vertigo. In fact, it is usually the onset of an anxiety state for a variety of reasons, in which balance discomfort predominates.
This is not a trivial observation. Patients who have endured chronic, medically unexplained dizziness often develop secondary anxiety, which then amplifies the perception of dizziness—creating a self‑sustaining loop. Conversely, patients with primary panic disorder or GAD frequently experience dizziness as a somatic symptom of the psychiatric condition itself.
A 2022 Johns Hopkins study found that the presence of dizziness symptoms like vertigo or light‑headedness was not significantly different between patients with organic vestibular disorders and those with psychiatric causes. The study concluded that assessment of psychiatric and autonomic symptoms should accompany, not follow, otologic evaluation of dizziness. This is a crucial clinical directive: the psychiatric assessment should run in parallel with the medical work‑up, not wait until the medical work‑up is “negative.”
For coding purposes, when dizziness is a recognised component of a psychiatric disorder—such as panic attacks (F41.0) in which dizziness is a listed symptom, or generalised anxiety disorder (F41.1) in which somatic anxiety symptoms include dizziness—the primary diagnosis is the psychiatric disorder, and R42 is not coded separately. The CDC official guidelines state that if dizziness is a component of the mental health condition, the dizziness is not coded separately; however, if dizziness is unrelated to the mental health condition, separate codes may be assigned for both.
Persistent Postural‑Perceptual Dizziness: The Bridge Diagnosis
The most significant recent advance in the understanding of chronic dizziness has been the formal recognition of persistent postural‑perceptual dizziness (PPPD) . First included in the ICD‑11 beta draft in 2015, PPPD is a chronic vestibular disorder characterised by persistent dizziness, unsteadiness, or non‑spinning vertigo lasting for more than three months, which is exacerbated by upright posture, walking, motion, or exposure to moving or complex visual stimuli.
PPPD unifies key features of what were previously described as chronic subjective dizziness, phobic postural vertigo, visual vertigo, and space‑motion discomfort. It is a functional neuro‑otologic disorder—neither purely organic nor purely psychogenic, but arising from the interaction between vestibular dysfunction and psychological processing.
The diagnostic criteria are now well established: one or more symptoms of dizziness, unsteadiness, or non‑spinning vertigo are present on most days for three months or more. Symptoms are provoked by upright posture, active or passive movement, or exposure to moving visual stimuli. The disorder is not better accounted for by another medical or psychiatric condition, though it may co‑occur with anxiety or depression.
For the mental health clinician, PPPD occupies the grey zone. It explains the patient who developed dizziness after an acute vestibular event (e.g., labyrinthitis or a panic attack) and whose symptoms persisted long after the initial trigger resolved. The treatment is often multidisciplinary, including vestibular rehabilitation, cognitive‑behavioural therapy (CBT), and sometimes SSRIs. Importantly, PPPD is coded with a neurological code—H81.9 (Unspecified disorder of vestibular function) or a more specific vestibular code when the diagnostic criteria are met—not with R42 and not with a psychiatric code unless a comorbid mental disorder is also present.

Somatic Symptom Disorder and Dizziness
When a patient presents with chronic, medically unexplained dizziness accompanied by disproportionate and persistent thoughts about the seriousness of the symptom, high levels of health anxiety, and excessive time and energy devoted to the symptom, the appropriate diagnosis may be F45.1 (Undifferentiated somatoform disorder) in ICD‑10, which maps to somatic symptom disorder in DSM‑5.
In this clinical picture, the dizziness is real; the patient is not “imagining” it. The pathological element is the cognitive‑affective response to the sensation—the conviction that the dizziness indicates a serious undiagnosed illness, the compulsive checking of balance, the avoidance of activities that might trigger the sensation.
The diagnostic threshold for F45.1 requires that the somatic symptoms be persistent (typically more than six months) and cause significant impairment in functioning. When this threshold is met, the primary diagnosis is F45.1, and R42 may be used as a secondary symptom code. The CDC guidelines note that if dizziness is unrelated to the mental health condition, separate codes may be assigned for both—but when the dizziness is the somatic expression of the psychiatric disorder, the psychiatric code should be primary.
The official Excludes2 note under R42 explicitly lists “psychogenic dizziness (F45.8)” as a separate diagnosis. F45.8 (Other somatoform disorders) is a billable code that includes somatoform autonomic dysfunction and psychogenic dysmenorrhoea. Psychogenic dizziness with no identified organic cause is properly coded here, not under R42.
Panic Disorder, GAD, and the Dizziness Symptom
Dizziness is a recognised somatic symptom of several anxiety disorders. The ICD‑10 descriptions explicitly include it:
F41.0 (Panic disorder [episodic paroxysmal anxiety]) : The essential feature is recurrent attacks of severe anxiety (panic). As with other anxiety disorders, panic attacks include symptoms such as palpitations, chest pain, choking sensations, dizziness, and feelings of unreality (depersonalisation or derealisation). During a panic attack, dizziness may be accompanied by rapid heartbeat, shaking, shortness of breath, and fear of death.
F41.1 (Generalised anxiety disorder) : Patients suffer from somatic anxiety symptoms including tremor, palpitations, dizziness, nausea, muscle tension, etc., as well as difficulty concentrating, nervousness, insomnia, and other psychic symptoms.
F40.01 (Agoraphobia with panic disorder) : Dizziness may be part of the symptom complex that leads to avoidance of situations from which escape might be difficult.
When a patient meets full diagnostic criteria for one of these disorders and dizziness is a component of the anxiety symptomatology, the primary diagnosis is the anxiety disorder, and R42 is not coded separately. The dizziness is not an independent condition; it is a manifestation of the underlying psychiatric illness.
The coding rule is straightforward: if the dizziness occurs only during panic attacks and is absent between attacks, it is not a separate diagnosis. If the patient experiences dizziness outside of panic attacks and the dizziness is not attributable to the anxiety disorder, separate coding may be justified—but the documentation must support the distinction.
Documentation: R42 as a Provisional vs. Definitive Code
From the mental health clinician‘s perspective, R42 serves several legitimate functions:
1. Provisional symptom coding during diagnostic work‑up. A patient presents with dizziness and anxiety, but it is not yet clear whether the dizziness is primary or secondary. While the patient is undergoing neurological or vestibular evaluation, R42 can be used as a secondary code alongside a provisional psychiatric diagnosis.
2. Concurrent coding when dizziness is documented without a specific underlying condition. The CDC guidelines state that if dizziness is not a component of the mental health condition (e.g., dizziness is unrelated to bipolar disorder), then separate codes may be assigned for both dizziness and the mental health condition. This requires explicit documentation that the two conditions are independent.
3. R42.81 for light‑headedness. When the patient‘s complaint is specifically light‑headedness rather than general dizziness, the more specific subcode R42.81 should be used. This is particularly relevant for anxiety‑related hyperventilation, in which light‑headedness is the dominant sensation.
4. Dizziness complicating pregnancy. For pregnant patients who experience dizziness, O26.892 (Dizziness complicating pregnancy) is used as the primary code, with R42 as a secondary code, if no specific vestibular diagnosis is established.
When R42 should NOT be the primary code:
A specific vestibular diagnosis has been made (e.g., BPPH, vestibular neuritis, Ménière‘s disease). Code the specific neurological or otologic condition.
Dizziness is a recognised component of a panic or anxiety disorder and occurs only in that context. Code the psychiatric disorder as primary.
PPPD has been diagnosed. Code the specific vestibular disorder (H81.x).
When R42 may be appropriate as a secondary code alongside a psychiatric primary diagnosis:
The patient has a confirmed psychiatric disorder (e.g., F41.1 GAD) and also reports dizziness that is not clearly part of the anxiety symptomatology. The documentation must state that the dizziness is unrelated to the mental health condition or occurs independently of anxiety episodes.
The patient is in the diagnostic grey zone where a vestibular disorder is suspected but not yet confirmed, and psychiatric symptoms are present. R42 can be used provisionally.
The documentation must always include the clinical reasoning that justifies the code choice. A note that says “patient dizzy” is insufficient. A note that says “patient reports light‑headedness between panic attacks, which is not a component of the panic symptomatology; neurological work‑up pending” supports the use of separate codes.
Frequently Asked Questions (FAQ)
1. When is R42 appropriate for a patient with anxiety and dizziness?
R42 is appropriate when the dizziness is not a recognised component of the anxiety disorder or when the dizziness occurs independently of anxiety episodes. For panic disorder with dizziness during panic attacks, the primary diagnosis is the anxiety disorder; R42 is not coded separately. For GAD with dizziness as a somatic symptom, the primary diagnosis is GAD; R42 is not coded separately. Only when the dizziness is unrelated to the mental health condition—and documentation supports that claim—should separate codes be used.
2. What is the difference between coding R42 and coding F45.8 (psychogenic dizziness)?
R42 is a symptom code used when the cause is unspecified. F45.8 (Other somatoform disorders) includes psychogenic dizziness—dizziness that is determined to be of psychological origin with no identified organic cause. If a thorough medical work‑up has excluded organic aetiology and the dizziness is judged to be a somatic expression of psychological distress, F45.8 is the more specific code. R42 is for dizziness with unknown aetiology; F45.8 is for dizziness with known psychological aetiology.
3. Can R42 be used as a primary diagnosis for reimbursement?
Yes, R42 is a billable, specific code that can be used as a primary diagnosis for reimbursement. However, it is a symptom code. Payers expect that the use of a symptom code will be followed by a diagnostic work‑up. Persistent use of R42 without evidence of evaluation for underlying causes may be questioned in audits.
4. How should I document dizziness in a patient with PPPD?
PPPD is a specific vestibular disorder. If the patient meets the diagnostic criteria (≥3 months of non‑spinning dizziness or unsteadiness provoked by upright posture, walking, or motion), the appropriate code is from the H81 range (e.g., H81.9 Unspecified disorder of vestibular function). R42 may be used as a secondary code if the documentation indicates that the specific vestibular diagnosis is not yet established. Psychiatric comorbidities (anxiety, depression) should be coded separately with their own F codes.
5. Does the Excludes2 note for psychogenic dizziness (F45.8) mean I cannot use R42 and F45.8 together?
No. Excludes2 notes indicate that the two conditions are not part of the same entity but can be used together if the patient has both diagnoses. If a patient has both psychogenic dizziness (F45.8) and an unrelated episode of general dizziness (R42) with a different cause, both codes can be assigned. However, if the dizziness is the psychogenic dizziness, F45.8 should be the primary code and R42 should not be used.
References
ICD‑10 Data. (2026). 2026 ICD‑10‑CM Diagnosis Code R42: Dizziness and giddiness.
ICDcodes.ai. (2026). Dizziness – ICD‑10 Documentation Guidelines.
S10.ai. (2025). ICD‑10 Coding for Lightheadedness (R42.81, I95.1).
Gesund.bund.de. (2025). ICD‑10 Code F41.1: Generalised anxiety disorder.
NCBI. (2025). Persistent Postural-Perceptual Dizziness (PPPD).
Vestibular First. (2025). Persistent Postural Perceptual Dizziness (PPPD).
If you’re ready to spend less time on documentation and more on therapy, get started with a free trial today
Not medical advice. For informational use only.
Outline
More articles





