The Therapy Roadmap: A Complete Guide to Writing Effective, Compliant Treatment Plans

May 20, 2026
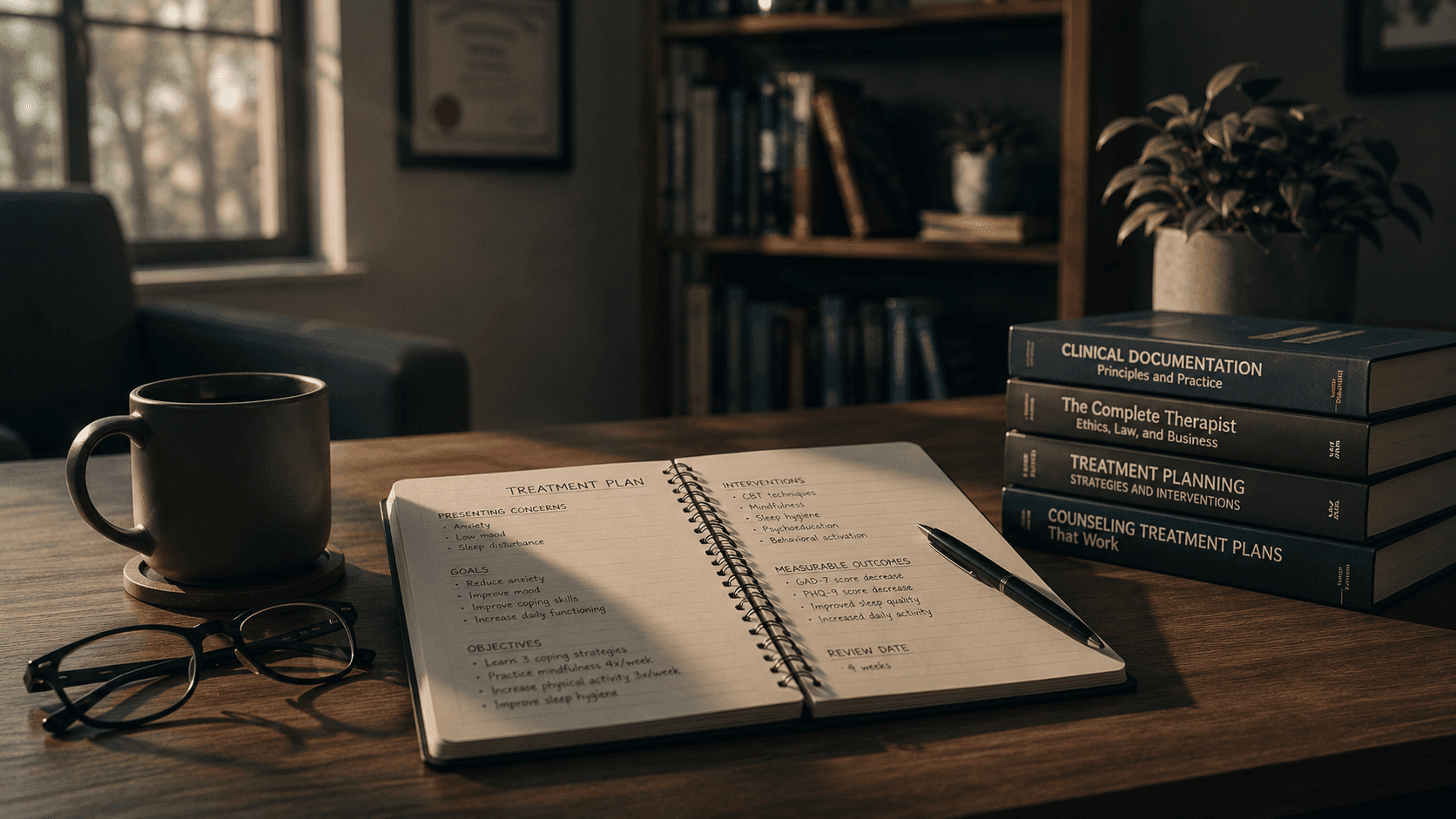
For mental health professionals, the therapy session itself is the heart of clinical work. But the treatment plan is the circulatory system—it gives the work direction, justifies its medical necessity, and ensures continuity when care is transferred or reviewed. A well‑constructed treatment plan is not merely administrative paperwork; it is a clinical tool that sharpens focus, aligns therapist and client around measurable goals, and serves as a legal and ethical record of the care provided.
This guide moves beyond templates and checklists. It offers a deep, practical framework for writing treatment plans that are clinically sound, audit‑ready, and genuinely useful for guiding therapy.
Why a Treatment Plan Matters Beyond the Filing Cabinet
Many clinicians view the treatment plan as a bureaucratic hurdle—something required by insurance companies but disconnected from the actual work of helping clients. This perspective undervalues the plan‘s true functions.
Clinical quality. A structured plan provides clear objectives and a systematic approach to therapy, enhancing the quality of care. It transforms vague intentions (“help client feel better”) into actionable targets (“reduce PHQ‑9 score from 22 to 12 within 12 weeks”).
Continuity of care. Treatment plans allow another clinician, supervisor, or case manager to quickly understand where the client is in treatment and what approaches have been effective so far. If you become unavailable, the plan ensures seamless continuation.
Insurance and audit defense. Insurance companies, managed care organizations, and licensing boards frequently require an up‑to‑date treatment plan to justify medical necessity and demonstrate progress. A well‑maintained plan shows that therapy is goal‑oriented, evidence‑based, and continuously evaluated, protecting both the therapist and the client in case of audits or peer reviews.
Therapeutic alliance. When clients participate in creating their treatment plan, the process builds trust, makes therapy goals transparent, and promotes shared responsibility for progress. The plan becomes a collaboration, not an imposition.
The Core Components of Any Treatment Plan
Most accrediting bodies and state behavioral guidelines converge on a set of core sections that every treatment plan must include. The table below breaks them down:
Component | What It Includes | Why It Matters |
|---|---|---|
Client Information & Assessment | Demographics, presenting concerns, psychosocial history, risk factors, strengths, functional impairments | Provides clinical context and grounds the treatment plan in a full biopsychosocial understanding |
Diagnosis (DSM‑5 / ICD‑10) | Formal DSM‑5‑TR or ICD‑10 diagnosis linked directly to assessed symptoms | Establishes medical necessity and anchors goals and interventions in recognized diagnostic criteria |
Problem List | A prioritized list of the primary issues the client is facing, informed by severity, functional impact, and the client‘s personal priorities | Ensures treatment focuses on what matters most |
Long‑Term Treatment Goals | Broad, outcome‑focused goals targeting symptom reduction and functional improvement | Clarifies the overall direction of care and communicates intended clinical outcomes |
Short‑Term Objectives | Specific, measurable, time‑bound steps that support each long‑term goal | Makes progress observable and supports outcome monitoring and insurance review |
Clinical Interventions | Evidence‑based techniques, therapeutic modalities, session frequency, and duration | Demonstrates clinical rationale and ensures interventions are appropriate for the diagnosis |
Timeline & Progress Measures | Concrete methods to assess progress (e.g., standardized assessment tools, self‑reports, behavioral observations) and a schedule for review | Provides accountability and shows whether the treatment is working |
Crisis / Safety Plan | Steps for managing risk, emergency contacts, warning signs, coping strategies | Protects client safety and demonstrates responsible risk management |
Consent & Confidentiality | Informed consent, treatment agreement, documentation of confidentiality limits | Ensures ethical practice and compliance with legal and professional standards |
From Broad Goals to Actionable Objectives: Mastering SMART
The most common weakness in treatment plans is vague goal language. A goal like “client will reduce anxiety” is clinically directionless and fails to satisfy auditors. The solution is the SMART framework, which transforms intentions into measurable targets.
Specific: Clearly define what you want to accomplish
Measurable: Identify concrete criteria for measuring progress
Achievable: Ensure the goal is realistic given the client‘s circumstances
Relevant: Align the goal with the client’s overall treatment needs
Time‑bound: Set a specific timeframe for achieving the goal
Before and After: SMART in Practice
Domain | Non‑SMART Goal | SMART Goal |
|---|---|---|
Anxiety | “Reduce anxiety symptoms” | “Client will reduce self‑reported anxiety severity from 8/10 to 4/10 within 6 weeks, as measured by weekly SUDS ratings and the GAD‑7 reassessment.” |
Depression | “Improve mood” | “Client will reduce PHQ‑9 score from 22 to 12 or lower within 12 weeks through weekly CBT sessions and daily behavioral activation exercises.” |
PTSD | “Reduce trauma symptoms” | “Client will decrease PCL‑5 score from 58 to 30 within 30 weeks by engaging in weekly or fortnightly EMDR sessions and completing assigned between‑session grounding exercises.” |
Step‑by‑Step: How to Build a Treatment Plan
Step 1: Gather Comprehensive Client Data
Begin with a thorough intake assessment. Collect presenting concerns, psychosocial history, risk factors, strengths, and functional impairments. Use standardized tools—PHQ‑9 for depression, GAD‑7 for anxiety, PCL‑5 for trauma—to establish a baseline and provide objective progress measures.
Step 2: Formulate a Precise Diagnosis
Assign a DSM‑5‑TR or ICD‑10 diagnosis linked directly to the assessed symptoms. The diagnosis establishes medical necessity and anchors all subsequent goals and interventions. Wisconsin Medicaid requirements, for example, specify that a treatment plan must be developed based on the initial evaluation and include measurable goals and expected outcomes.
Step 3: Develop a Prioritized Problem List
Identify the primary issues the client is facing. Prioritize by severity of symptoms, impact on daily functioning, and the client‘s own goals. This list becomes the backbone of the treatment plan.
Step 4: Write SMART Short‑Term Objectives
Break each long‑term goal into specific, measurable steps. For a client with social anxiety, objectives might include:
“Client will identify three specific anxiety triggers in social situations within two sessions.”
“Client will attend one low‑risk social gathering per week for four consecutive weeks, rating anxiety pre‑ and post‑event.”
Step 5: Select Evidence‑Based Interventions
Choose therapeutic modalities that are appropriate for the diagnosis and tailored to the client‘s circumstances. For GAD, first‑line interventions include CBT targeting cognitive distortions, psychoeducation on anxiety physiology, relaxation techniques, and mindfulness skills.
Document the frequency and duration of sessions (e.g., “weekly 50‑minute individual CBT sessions for 12 weeks”) to support insurance review.
Step 6: Establish Progress Measures and Timeline
Specify how you will assess progress: repeat standardized assessments at regular intervals, track symptom logs, or monitor behavioral frequency counts. Set a schedule for reviewing the treatment plan—ideally at least every 30 to 90 days, or more frequently if the client‘s status changes.
Step 7: Draft a Crisis / Safety Plan
For any client with safety concerns (suicidality, self‑harm, aggression risk), include a crisis plan with warning signs, coping strategies, emergency contacts, and steps for escalating care. This not only protects the client but also demonstrates risk management to auditors.
Step 8: Review and Revise Collaboratively
The treatment plan is a living document. Review it with the client, explain each section, and invite their input. A plan imposed without collaboration leads to disengagement. Update the plan whenever there is a significant change in symptoms, functioning, or life circumstances.
Common Mistakes and How to Avoid Them
Mistake | Why It‘s a Problem | The Fix |
|---|---|---|
Vague goals | Auditors cannot assess progress; therapy drifts | Use SMART criteria; include specific numerical targets |
Ignoring client input | Weak therapeutic alliance; low treatment adherence | Review the plan with the client; adjust based on their priorities |
Copy‑forwarding old plans | Auditors detect “template care“; no evidence of individualized treatment | Update the plan each review period; document changes explicitly |
Failing to link interventions to diagnosis | Medical necessity is not justified | For each intervention, state how it addresses the specific diagnosis |
No discharge planning | Treatment may end abruptly without preparation | Include a discharge section: criteria for termination, anticipated duration, aftercare recommendations |
Missing progress measures | No data to support continued authorization | Schedule regular reassessments; document scores and functional changes |
Integrating Treatment Plans with Progress Notes
A treatment plan is not a standalone document. It must connect directly to your daily progress notes. Every progress note should reference the plan: identify which goal or objective was addressed, describe the intervention used, document the client‘s response, and note progress toward the objective. This “golden thread” of documentation—linking problem → goal → intervention → response → progress—is what auditors expect and what justifies medical necessity.
Treatment Plan Examples by Diagnosis
Generalized Anxiety Disorder (GAD)
Diagnosis: F41.1 (ICD‑10)
Long‑Term Goal: Reduce generalized anxiety symptoms and improve emotional regulation and daily functioning.
Short‑Term Objectives: (1) Client will reduce self‑reported anxiety from 8/10 to 4/10 within 6 weeks. (2) Client will identify three primary worry triggers within 4 sessions. (3) Client will practice a grounding or relaxation exercise daily for 10 minutes for 4 weeks.
Interventions: Weekly CBT targeting cognitive distortions, psychoeducation on anxiety physiology, relaxation training, mindfulness skills, and referral for psychiatric evaluation if needed.
Major Depressive Disorder (MDD)
Diagnosis: F32.9 (ICD‑10)
Long‑Term Goal: Reduce depressive symptoms and restore daily functioning.
Short‑Term Objectives: (1) Client will lower PHQ‑9 score from 22 to ≤12 within 12 weeks. (2) Client will schedule and attend three pleasant activities per week for 4 weeks. (3) Client will identify and challenge three negative automatic thoughts per week using a thought record.
Interventions: Weekly CBT with behavioral activation, psychoeducation on the cognitive model, structured problem‑solving, and sleep hygiene protocol.
PTSD
Diagnosis: F43.10 (ICD‑10)
Long‑Term Goal: Reduce trauma‑related symptoms and improve emotion regulation.
Short‑Term Objectives: (1) Client will decrease PCL‑5 score from 58 to ≤30 within 30 weeks. (2) Client will utilize two grounding techniques to manage flashbacks, rating effectiveness weekly.
Interventions: Weekly EMDR or prolonged exposure therapy, between‑session bodywork, grounding skill training, and psychoeducation on trauma responses.
Preparing for Insurance and Regulatory Audits
Auditors scrutinize treatment plans for specific elements:
Current, covered diagnosis (active ICD‑10 code)
Measurable, individualized goals (not copied from a template)
Specific interventions (not vague “counseling”)
Progress measures and review dates
Client signature or documented agreement
Documentation checklist for audit readiness:
Diagnosis is clearly stated and linked to symptoms.
Each long‑term goal is paired with SMART short‑term objectives.
Interventions are evidence‑based and matched to the diagnosis.
Review schedule is specified (e.g., “every 30 days”).
The plan is signed and dated by the treating clinician.
The client has reviewed and agreed to the plan (signature or notation).
FAQ
How often should a treatment plan be updated?
At a minimum, review the plan every 30 to 90 days, or whenever the client‘s status changes significantly. Some payers require a formal update every 90 days for continued authorization.
Do all payers require a treatment plan?
Yes, virtually all insurance companies, Medicaid, Medicare, and managed care organizations require a current treatment plan to justify medical necessity. Without a plan, claims may be denied.
What‘s the difference between a long‑term goal and a short‑term objective?
A long‑term goal is a broad outcome expected from the course of therapy (e.g., “reduce depressive symptoms”). Short‑term objectives are specific, measurable, time‑bound steps that demonstrate progress toward the long‑term goal (e.g., “client will reduce PHQ‑9 score by 50% within 8 weeks”).
Can I use the same treatment plan for two clients with the same diagnosis?
No. While the structure and intervention categories may be similar, the plan must be individualized. Different clients have different specific symptoms, functional impairments, strengths, and personal goals. Auditors reject identical “template” plans.
How do I document a client who refuses to participate in treatment planning?
Document the refusal explicitly. Note what you explained about the plan, what they declined to do, and that you will make the plan available for their review. Proceed to write the plan based on your clinical assessment, but keep the door open for later collaboration.
Conclusion
The treatment plan is not a burden to be rushed through between sessions. It is the strategic core of therapy—a document that clarifies purpose, coordinates care, demonstrates accountability, and, most importantly, centers the work on what the client actually needs to change. A well‑written treatment plan makes the difference between drifting from week to week and moving systematically toward measurable, meaningful outcomes.
Mastering treatment planning is an investment that pays dividends in clinical focus, client engagement, audit security, and professional confidence. Start with the template that fits your practice, commit to the SMART framework, and review your plans as living documents—not museum pieces—and you will transform documentation from a chore into an asset.
References
ForwardHealth Wisconsin. (2026). Program Requirements – Adult Mental Health Day Treatment.
Behave Health. (2026). Treatment Plan Templates & Examples (2026).
Behave Health. (2026). Progress Notes Examples & Templates (2026).
Medicare Consulting for Therapists. (2024). How to Prepare for Insurance Audits.
If you’re ready to spend less time on documentation and more on therapy, get started with a free trial today
Not medical advice. For informational use only.
Outline
More articles





