
May 14, 2026
In the cognitive model, symptoms do not arise in a vacuum. Beneath every episode of depression, every spike of anxiety, every compulsive ritual lies a layer of cognition — not always accessible, not always rational, but consistently organized in predictable ways. The task of cognitive therapy is not merely to challenge negative thoughts when they appear, but to map the architecture of thinking that generates them. That mapping process is case conceptualization, and for the practicing clinician, it is the single most important tool for transforming raw clinical data into a coherent, actionable treatment plan. This article examines the structure, the methods, and the common pitfalls of cognitive conceptualization, with the goal of equipping therapists to build formulations that are precise, collaborative, and genuinely useful.
The Core Layers – Why Distal Beliefs Matter
The cognitive model conceptualizes the mind as a hierarchical structure of knowledge. At the surface are automatic thoughts, the fleeting verbal or imaginal cognitions that accompany emotional distress. At the deepest level are core beliefs, the absolutist, global, and overgeneralized assumptions about self, others, and the world that colour an individual‘s entire experience. Connecting these two levels are intermediate beliefs – attitudes, rules, and conditional assumptions that specify how an automatic thought is derived from a core belief.
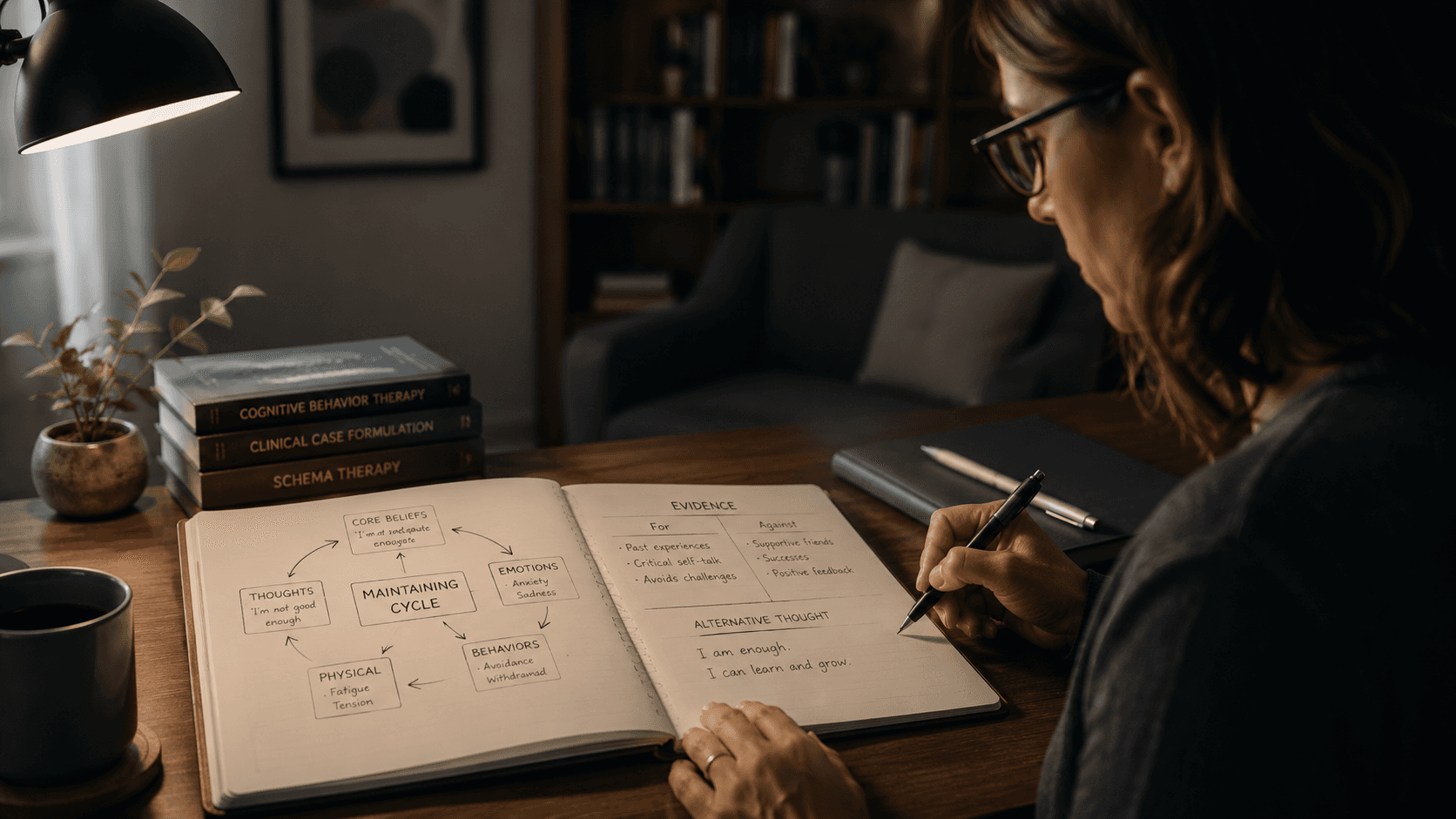
In anxiety, a core belief of vulnerability may be expressed as a conditional assumption: “If I go out alone, something terrible will happen.” That assumption, in turn, generates automatic thoughts: “That man is following me.” In depression, a core belief of defectiveness generates conditional beliefs such as “If I am criticized, it proves I am worthless,” leading to automatic thoughts of “I am a failure.” The cognitive conceptualization diagram (CCD) developed by Judith Beck arranges these three levels into a single visual representation, linking them to relevant early life experiences that shaped them and to the specific situations that activate them now.
The clinical utility of this hierarchical model lies in its stability gradient. Automatic thoughts shift easily. Core beliefs are the most stable and the most difficult to modify directly. Case conceptualization helps the therapist identify which level is driving a client’s difficulties and plan treatment accordingly. More critically, it prevents the common error of treating surface symptoms without ever addressing the underlying structures that generate them.
The Early Origins of Beliefs
Cognitive conceptualization is longitudinal in design. The CBT approach to case formulation, largely based on Beck’s cognitive model, posits that core beliefs are the product of early childhood experiences — repeated patterns of reinforcement or punishment, interactions with attachment figures, and the gradual internalization of an understanding of self and others. The conceptualization diagram explicitly includes a section for relevant childhood information that gives rise to the core beliefs identified in the diagram. The expectation is not that a therapist can reconstruct a complete developmental history, but that enough historical data can be gathered to establish a plausible, clinically useful etiological hypothesis.
Research has validated the importance of early adverse experiences in the formation of maladaptive schemas and supports the core assumptions of Beck's cognitive model. Early neglect, abuse, or persistent criticism produce systematic patterns of overgeneralization. A child who is told repeatedly that she is “stupid” does not merely experience momentary hurt; she builds a core belief about her own intelligence that persists into adulthood, even when all objective evidence contradicts it. The clinician who fails to uncover that early history may misinterpret the client‘s reluctance to trust or take risks as resistance, rather than as a logical consequence of a developmental script.
The Building Blocks of a Conceptualization – Three Levels of Cognition
A fully developed cognitive conceptualization integrates three levels of cognition. The most common method for constructing a conceptualization is the Cognitive Conceptualization Diagram, which graphically organizes data into a hypothesis about the origins, activation, and maintenance of a client’s problems.
Automatic Thoughts
Automatic thoughts are the most accessible level of cognition. They are not derived from conscious inference; they appear spontaneously, often in shorthand form (“He hates me,” “I can‘t do this”), and they are typically accepted as true without evaluation. In practice, automatic thoughts are best elicited using the “downward arrow” technique, in which the therapist repeatedly asks, “If that were true, what would it mean about you?” This technique moves from the surface thought to the meaning underlying it.
Clinically, the presence of automatic thoughts is not itself pathological. It is the content, frequency, and believability of these thoughts that distinguishes adaptive from maladaptive functioning.
Intermediate Beliefs
Intermediate beliefs are the rules, attitudes, and assumptions that link automatic thoughts to core beliefs. They often take the form of conditional “if–then” statements: “If I don‘t perform perfectly, then I am a failure” or “If someone criticizes me, it means they hate me.” These beliefs are activated in specific domains—work, relationships, academic performance —but may not generalize across all situations.
In cognitive conceptualization, intermediate beliefs can be the most productive targets for initial intervention because they are more accessible than core beliefs but more stable than automatic thoughts. Modifying an intermediate belief does not require full restructuring of the core belief system, but it can significantly reduce the frequency of problematic automatic thoughts.
Core Beliefs
Core beliefs are the deepest level of the cognitive hierarchy. They are unconditional, global, and abstract statements about the self, others, and the world: “I am unlovable,” “I am incompetent,” “Others are dangerous,” “The world is unfair.” These beliefs are typically learned early in development and, once formed, function as a cognitive filter: the person selectively attends to information that confirms the belief and discounts or distorts information that contradicts it. A person who believes “I am unlovable” will interpret a partner‘s neutral expression as rejection and dismiss a partner’s affection as temporary or insincere.
The stability of core beliefs presents a therapeutic challenge. They are not easily modified by direct disputation or positive affirmations. Instead, cognitive therapy works to establish new, more adaptive core beliefs through the accumulation of contradictory evidence over time, often supported by behavioural experiments that test the predictions of both the maladaptive and the adaptive belief.

The Cross-Sectional vs. Longitudinal Diagram – A Strategic Choice
The Cognitive Conceptualization Diagram exists in two versions: a cross-sectional diagram that captures the current relationship among automatic thoughts, emotions, behaviors, and situations; and a longitudinal diagram that adds the historical dimensions of childhood origins and core beliefs. The choice between them is strategic.
The cross-sectional diagram is invaluable in the early stages of therapy when the goal is to help the client understand the cognitive model and to build a shared formulation of the problem. It is also useful when the client’s difficulties appear to be reactive to specific situations without a deeply entrenched core belief structure. The longitudinal diagram is reserved for cases in which the client‘s difficulties are chronic, recurrent, or clearly tied to longstanding patterns — most obviously, for clients with personality disorders or complex trauma. For these clients, a formulation that does not address the distal origins of their beliefs will feel incomplete and may undermine the credibility of the therapist.
Case Conceptualization as an Ongoing Process
Case conceptualization in cognitive therapy is not a one‑time event. It is a dynamic, iterative process that begins before the first session and continues through termination.
In the first session, the conceptualization is necessarily provisional, based on limited information. As therapy progresses, new data emerges—the client’s reaction to interventions, the emergence of previously unreported patterns, the in‑session dynamics between therapist and client. Each new data point requires the therapist to revise and refine the formulation. The conceptualization that guides termination should be far more precise, individualized, and nuanced than the one that guided the first session.
This is not a weakness of the formulation process; it is its strength. A static formulation is a dogmatic one, and dogmatism is the enemy of effective psychotherapy. The best formulations retain a degree of provisionality, always open to disconfirmation, always willing to accommodate new information. The metaphor of the formulation as a “map” is appropriate here: the map is useful only insofar as it corresponds to the territory. When the territory changes, the map must change as well.
Content‑Specificity – The Differential Signature of Depression and Anxiety
Beck‘s cognitive model predicts that depressed and anxious individuals can be differentiated on the basis of their cognitions regarding their self, world, and future. Depression is characterized by the negative cognitive triad: the depressed person views the self as defective or inadequate, the world as obstructive or punishing, and the future as hopeless. Anxiety, by contrast, is characterized by cognitions of threat, unpredictability, and loss of control.
These differences are not merely theoretical; they have been empirically demonstrated across dozens of studies. Depressed individuals show a specific memory bias for negative, depression‑relevant stimuli, whereas anxious individuals show a bias for threat‑related stimuli. A conceptualization that fails to capture these content differences will be imprecise. More important, it may lead to generic interventions—cognitive restructuring focused on “negative thinking” in general—rather than the targeted strategies that address the specific content of each disorder.
When anxiety and depression co‑occur, which they often do, the conceptualization must identify the relative contribution of each cognitive profile. Is the client primarily depressed with secondary anxiety, or is the anxious preoccupation the driver of the depressive symptoms? The treatment implications are significant, and the formulation is the tool that answers the question.
Cultural Competence in Cognitive Conceptualization
Cognition is fundamentally cultural. The beliefs that constitute a core belief are not formed in a cultural vacuum; they are acquired from family, community, religious institutions, and the broader society. A cognitive conceptualization that ignores cultural context is not merely incomplete; it is likely to be actively misleading.
Consider a client from a collectivist culture who expresses the belief that she must subordinate her own needs to those of her family. In an individualist framework, this might be interpreted as a maladaptive core belief of worthlessness or an inability to prioritize one‘s own needs. Within the client’s cultural context, it may be an accurate reflection of a core cultural value. The distinction is critical. The goal of cognitive therapy is not to eliminate culturally congruent beliefs; it is to help the client evaluate the usefulness of their beliefs in achieving their own goals.
Similarly, the expression of distress itself is culturally shaped. In some cultures, psychological distress is somatized; in others, it is externalized as anger or relational conflict. The culturally competent therapist adapts the formulation to the client’s idiom of distress, not imposing Western diagnostic categories onto non‑Western presentations.
Common Errors and How to Avoid Them
Over‑inference
The most common error in cognitive conceptualization is drawing conclusions from insufficient data. A single instance of automatic negative thinking does not constitute a core belief. Intermediate beliefs are identified only after observing consistent patterns across multiple situations.
The remedy is disciplined data collection. Use the cognitive conceptualization diagram as a hypothesis‑generating tool, not a final verdict. When data contradict the formulation, the formulation is wrong—not the data.
Schematic Rigidity
Another error is using the same formulation structure for every client. The three‑level hierarchy of automatic thoughts, intermediate beliefs, and core beliefs is a useful heuristic, but not every client‘s difficulties conform neatly to this model. Some clients have difficulty identifying automatic thoughts; for them, a behavioural or experiential focus may be more productive early in therapy. Some clients present with problems that are primarily behavioral or interpersonal, with minimal cognitive content. The formulation should fit the client, not the other way around.
Confirmation Bias
A pervasive risk in case conceptualization is the tendency to seek evidence that confirms the formulation while ignoring evidence that disconfirms it. This is a cognitive error not limited to clients; therapists are equally susceptible. The antidote is systematic feedback collection. Present the formulation to the client explicitly and ask: “Does this fit your experience? What am I missing?” The client is the ultimate arbiter of the formulation‘s accuracy.
Challenges in Conceptualization – When Core Beliefs Are Ambiguous
Some clients present with patterns of difficulties that do not map neatly onto a single, stable core belief. The construct of a ‘core belief’ has been criticized as ill‑defined, and its ambiguity can create problems for the clinician. In such cases, a formulation that focuses on intermediate beliefs or behavioral patterns may be more productive than forcing the data into a core‑belief framework.
Similarly, clients with personality disorders may have multiple, contradictory core beliefs that are activated in different contexts. A person with borderline personality disorder may hold a core belief of “I am worthless” in some situations and “I am superior” in others. A formulation that captures this vacillation is more clinically useful than one that tries to reduce the client to a single, static belief.
The Therapeutic Relationship – The Medium of Formulation
The case conceptualization in CBT is developed collaboratively, not imposed by the expert therapist. The therapeutic relationship is central to the process of case conceptualization, and a strong therapeutic alliance is required for the development of a formulation that is both accurate and usable.
There is a growing recognition that alliance ruptures are reciprocal, with both client and therapist bringing expectations and beliefs to the interaction. A comprehensive cognitive conceptualization of the therapeutic relationship should include an assessment of both the client‘s and the therapist’s core beliefs and the ways in which they interact. For example, a therapist with a core belief that “I must be competent” may respond to a client‘s lack of progress with anxiety, which the client interprets as impatience, confirming the client’s core belief that “I am a burden.” The formulation that captures this interactional pattern opens the possibility of repair.
From Conceptualization to Intervention – The Strategic Plan
A conceptualization that does not guide intervention is an intellectual exercise, not a clinical tool. The primary purpose of the formulation is to inform treatment decisions: which level of belief to target first, which techniques to use, and how to sequence them.
Guidelines for translating the conceptualization into a treatment plan are well established. When the client’s difficulties are driven by automatic thoughts without a strong core belief structure, a focus on cognitive restructuring and behavioural activation may be sufficient. When a client‘s problems are maintained by rigid intermediate beliefs, interventions that target these assumptions—such as behavioural experiments designed to test the rule’s validity—may be most effective. When core beliefs are the primary driver, longer‑term strategies—including belief modification, continuum work, and historical testing of the evidence for and against the belief—are typically required.
The conceptualization also provides a guide for troubleshooting when therapy stalls. If a client fails to respond to an intervention, the formulation is the first place to look. Did we misidentify the level of the problem? Is there a hidden assumption that we have not yet addressed? Is there a cultural factor we failed to consider? The formulation does not just tell the therapist what to do; it tells them where to look when the plan is not working.
FAQ
What is the difference between a cognitive conceptualization and a psychiatric diagnosis?
A diagnosis places a client within a category (e.g., major depressive disorder, social anxiety disorder). A conceptualization explains why this particular individual, at this particular point in time, developed this particular pattern of difficulties. The conceptualization is idiographic; the diagnosis is nomothetic. Both are useful, but the conceptualization has far more treatment implications.
How long does it take to develop a complete conceptualization?
A preliminary conceptualization can often be developed during the first session, based on the client‘s presenting complaints and a brief developmental history. A full longitudinal conceptualization, including childhood origins and the relationship between core beliefs and current patterns, typically requires two to four sessions of data gathering. However, the conceptualization is never “complete” in the sense of being finished; it is continually revised as new information becomes available.
Can cognitive conceptualization be used with clients who have difficulty identifying their thoughts?
Yes. For clients who have difficulty accessing automatic thoughts, the therapist can begin with the behavioural or emotional level of the diagram. Once a problematic behaviour or emotion is identified, the therapist can work backward to the cognition that preceded it. Behavioural experiments and in‑session “experiments” (e.g., inducing a mild stressor) can also help bring automatic thoughts into awareness.
Is there research supporting the use of cognitive case conceptualization?
The evidence base for case conceptualization is mixed. Some reviews challenge its claimed benefits, pointing to variability in reliability and the lack of rigorous outcome studies. However, the cognitive conceptualization diagram (CCD) has demonstrated reliability across different levels of practitioner experience in controlled studies. Most experts agree that while the evidence base is incomplete, the clinical consensus strongly supports the use of formulation as an organizing framework.
How should I document a cognitive conceptualization in the medical record?
The conceptualization should be documented clearly enough that another clinician could understand the rationale for treatment. However, it is not typically entered verbatim into the medical record, where it may be misinterpreted by non‑CBT clinicians or by the client themselves. A summary of the formulation, with the core beliefs and intermediate beliefs listed, is appropriate. The detailed diagram and the therapist’s private hypotheses should be kept in the psychotherapy notes, which are not part of the designated record set and are not subject to release under HIPAA without the client‘s specific authorization.
References
If you’re ready to spend less time on documentation and more on therapy, get started with a free trial today
Not medical advice. For informational use only.
Outline
More articles





